Resident Physician Integris Baptist Medical Center Oklahoma City, Oklahoma, United States
Purpose: Insurance-driven administrative complexity contributes to physician burnout, rising healthcare costs, and fragmented care across specialties. Inefficiencies in primary care influence downstream utilization, including referrals, emergency care, and imaging. This study evaluates a subscription-based hybrid care model designed to remove insurers from routine care while preserving protection for high-cost medical events.
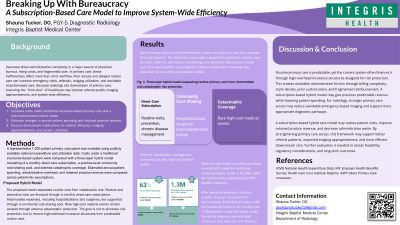
Methods/Materials: Using publicly available national expenditure and utilization data, we modeled a representative 1,000-patient primary care panel. Costs under a traditional insurance-based system were compared with a three-layer hybrid model consisting of a monthly direct-care subscription, a practice-level community cost-sharing pool for hospitalizations and surgeries, and external catastrophic coverage for rare high-cost events. Administrative overhead, patient spending, and retained practice revenue were estimated for both systems.
Results: Mean annual patient spending under the insurance-based model was estimated at $5,600 compared with $2,080 under the subscription-based model, representing a 63% relative reduction. After operating expenses, practices retained approximately $1.3 million annually per 1,000 patients under the hybrid model versus approximately $180,000 under traditional insurance. Sensitivity analyses demonstrated consistent cost reductions and financial stability across patient-mix assumptions.
Conclusions: A subscription-based hybrid care model substantially reduces patient costs and administrative waste while supporting predictable, relationship-based care. By improving access to primary care and reducing fragmented utilization, this framework may improve downstream imaging appropriateness, referral efficiency, and overall system performance. These findings support further evaluation of subscription-based models as a scalable strategy to improve care delivery and physician sustainability.