Medical Student (class of 2026) NYU Grossman School of Medicine New York, New York, United States
Purpose: To characterize diagnostic outcomes and safety implications following nondiagnostic (ND) endoscopic ultrasound-guided fine-needle aspiration (EUS-FNA) performed for pancreatic abnormalities detected on imaging.
Methods/Materials: Adult patients who underwent EUS-FNA for imaging-detected pancreatic abnormalities between 2020 and 2025 were retrospectively identified. Cases were included if the EUS-FNA result was nondiagnostic and excluded if definitive pathology was obtained from concurrent sampling, prior pancreatic cancer was present, or follow-up was less than one year. Imaging features were extracted from original CT, MRI, and PET reports, including lesion type, location, ductal dilation, and radiologic suspicion. A blinded radiologist independently re-reviewed imaging for concordance. EUS findings, laboratory values, and final outcomes (defined by histopathology or longitudinal clinical and imaging follow-up) were obtained from the electronic medical record. Associations were assessed using Fisher’s exact test with odds ratios (95% CI), and time to diagnosis was compared using the Wilcoxon rank-sum test.
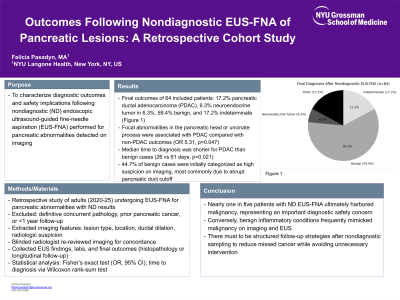
Results: Among 64 included patients (mean age 68.7 years), final outcomes were pancreatic ductal adenocarcinoma (PDAC) in 17.2%, neuroendocrine tumor in 6.3%, benign in 59.4%, and indeterminate in 17.2%. Focal abnormalities in the pancreatic head or uncinate process were associated with PDAC compared with non-PDAC outcomes (OR 5.31, p=0.047). Median time to diagnosis was shorter for PDAC than benign cases (26 vs 61 days, p=0.021). CA 19-9 was elevated in 90% of PDAC cases but also in 22.7% of benign cases, all attributed to pancreatitis. Notably, 44.7% of benign cases were initially categorized as high suspicion on imaging, most commonly due to abrupt pancreatic duct cutoff.
Conclusions: Nearly one in five patients with ND EUS-FNA ultimately harbored malignancy, representing an important diagnostic safety concern. Conversely, benign inflammatory conditions frequently mimicked malignancy on imaging and EUS, underscoring the need for structured follow-up strategies after nondiagnostic sampling to reduce missed cancer while avoiding unnecessary intervention.