Associate Professor University of California Irvine Orange, California, United States
Purpose: To assess resource utilization and screening eligibility among patients age 40 and older undergoing diagnostic breast imaging for breast pain alone, and to evaluate clinical characteristics and outcomes.
Methods/Materials: We retrospectively reviewed 671 patients age 40 and older without a history of breast cancer who underwent diagnostic breast imaging for breast pain alone at our institution from 1/2022 to 12/2022. Patients were considered eligible for screening if no prior mammograms were available in our system or their most recent bilateral mammogram was more than 12 months prior to presentation.
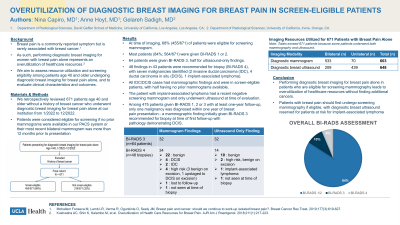
Results: In 671 patients with breast pain, 533 bilateral and 70 unilateral diagnostic mammograms and 209 bilateral and 439 unilateral diagnostic breast ultrasounds were performed. At time of imaging, 68% (455/671) of patients were eligible for screening mammogram. Most patients (564/671) were given BI-RADS 1 or 2. Sixty-four patients were given BI-RADS 3, nearly half for ultrasound-only findings. Forty-eight findings in 43 patients were recommended for biopsy (BI-RADS 4), with seven malignancies identified (2 IDC, 4 DCIS, 1 implant-associated lymphoma). One biopsy-proven high-risk lesion was upstaged to DCIS at excision. All IDC/DCIS cases had mammographic findings and were in screen-eligible patients, with half having no prior mammograms available. The patient with implant-associated lymphoma had a recent negative screening mammogram and only underwent ultrasound at time of evaluation. 13/48 biopsies were for benign ultrasound-only findings. Among 475 patients given BI-RADS 1, 2 or 3 with at least one-year follow-up, only one malignancy was diagnosed within one year of breast pain presentation - a mammographic finding initially given BI-RADS 3 recommended for biopsy at time of first follow-up with pathology demonstrating DCIS.
Conclusions: Performing diagnostic breast imaging for breast pain alone in patients who are eligible for screening mammography leads to overutilization of healthcare resources without finding additional cancers. Patients with breast pain should first undergo screening mammography, with diagnostic breast ultrasound reserved for patients at risk for implant-associated lymphoma.